Neurospine Institute has a conservative approach to patient management and we do not recommend surgery lightly. We offer management of all simple and complex spine surgical problems in the whole spine requiring either anterior or posterior surgical approaches for primary and revision spine surgery problems. We use conventional and Minimally Invasive Spine Surgery (MISS) techniques (‘Keyhole Surgery’) where appropriate.
For bookings or further information please phone on(08) 6147 8222or book an appointment below.
The team at Neurospine Institute utilise the latest neurosurgical techniques including
Computer assisted neuronavigation using the BrainLab System
Functional mapping of motor, sensory and language cerebral cortex using the Ojemann cortical stimulator
Awake Craniotomy techniques to further identify eloquent functional cerebral cortex
These techniques are used where appropriate in addition to standard neurosurgical techniques to help identify brain tumour margins, areas of important functional brain and their relationship to the tumour margins. This helps the surgeon maximise the tumour resection while minimising the risk of damage adjacent functional brain
Cerebral Metatases
Cerebral metastases are cancers that began elsewhere in the body and spread from their original site to the brain(‘secondary brain tumours”). They can form one or more tumours at different locations in the brain. Brain metastases are the most common brain tumours. They are more common than tumours that primarily originated in the brain (‘primary brain tumours’). A metastatic brain tumour can start as any cancer but more commonly as lung, breast, bowel, kidney,ovaries, testes, skin (melanoma) or blood cancer (‘lymphoma’). Sometimes the origin of the brain metastases is not known at the time of diagnosis.
Symptoms and signs can include headaches, nausea, vomiting, mental changes, seizures, paralysis, sensory, speech or visual deficits. Treatment for patients with cerebral metastases is often surgery, radiation or both. Chemotherapy and immunotherapy are sometimes effective. At the Neurospine Institute we work closely with other specialists, such as oncologists and haematologists and treat metastatic brain tumours in a multidisciplinary fashion to offer our patients the best possible outcome.
Computer Assisted/Neuro-navigated Brain Surgery
In cranial surgery, the very latest technology such as computer-assisted surgical navigation allows for planning and precise execution of needle biopsy and approach to brain lesions. The extent of tumour resection can be confirmed in the operating theatre before the end of surgery.
Awake Craniotomy
The safe removal of primary brain tumours depends on an understanding of the relationship of the tumour to functional brain regions such as those that enable movement, sensation and language. This is usually determined relatively easily pre-operatively on imaging modalities such as MRI, sometimes supplemented by advanced imaging techniques such as functional MRI which can readily identify motor and somatosensory cortex.
Fortunately, most brain tumours develop in the brain at a distance from brain regions important for functions such as movement, sensation and language. This allows removal of the tumour with a margin of normal white matter, a so called macroscopically complete resection, with a minimal risk of new neurological problems. This is very important as a maximal removal of gliomas (a type of tumour that occurs in the brain) is thought to be associated with an improved survival from what are often very malignant tumours.
Sometimes the proximity on MRI of a brain tumour to functional brain may potentially restrict resection to either biopsy alone or a limited incomplete resection, both of which may significantly worsen prognosis. In this setting, sometimes utilizing techniques such as cortical stimulation in an awake patient to identify important functional brain during tumour removal can demonstrate a degree of separation of tumour and functional brain not captured on pre-operative MRI that then allows a safe maximal tumour removal.
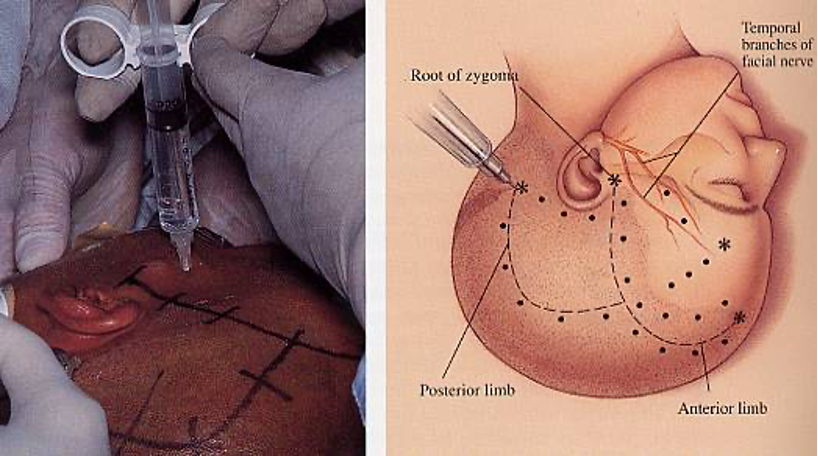
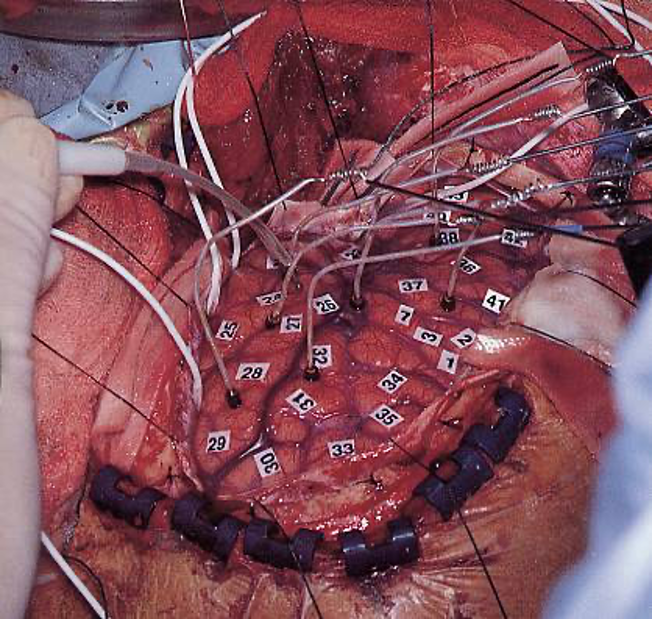
In an awake craniotomy, a combination of local anaesthetic infiltration of the scalp combined with IV sedation is used during opening of the skull and exposure of the brain. The IV sedation is then ceased and the patient allowed to awaken mid-procedure. As the brain itself has no pain sensation, surgical procedures can be performed on the brain in a conscious patient. Direct stimulation of the brain with a small electrical current then allows identification of functional cortex.
When motor cortex is stimulated, involuntary movements will occur. When somatosensory cortex is stimulated the patient will report changes in sensation to parts of the body. If language cortex is stimulated while the patient is speaking, speech arrest or dysphasic speech errors will occur.
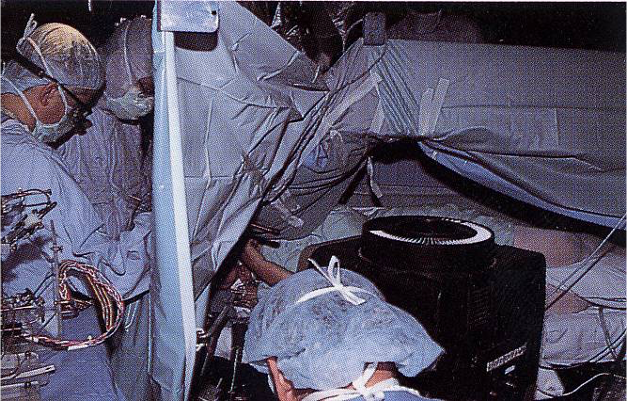
Dr Miles performing an awake craniotomy in 1990s
Neuro-oncology
The team at Neurospine Institute utilise the latest neurosurgical techniques including:
Computer assisted neuronavigation using the BrainLab System
Functional mapping of motor, sensory and language cerebral cortex using the Ojemann cortical stimulator
Awake Craniotomy techniques to further identify eloquent functional cerebral cortex
These techniques are used where appropriate in addition to standard neurosurgical techniques to help identify brain tumour margins, areas of important functional brain and their relationship to the tumour margins. This helps the surgeon maximise the tumour resection while minimising the risk of damage adjacent functional brain.
Cervical Disc Herniation
A cervical disc herniation, or cervical radiculopathy, occurs when a small portion of a disc ruptures and causes pressure on spinal nerves in the neck.
Small herniations are sometimes called bulges or protrusions, and people experiencing pain from the herniation often describe it as a pinched nerve.
Symptoms:
Depending on which cervical disc has herniated, the specific pain symptoms may vary. In general, pressure on a spinal nerve causes discomfort in various sites along one or both arms, frequently down to the hand. There can be shooting, burning pains, weakness, and/or numbness. In some instances, a cervical herniation can cause pressure on the spinal cord, a condition called cervical stenosis. Stenosis can lead to a medical condition called myelopathy. Myelopathy symptoms can include neck stiffness, numbness or heaviness in the arms and hands, or a shock-like feeling down the arms or legs. In severe cases, there can be difficulty using the arms and hands or difficulty walking.
Causes:
Cervical disc herniations are most frequently caused by degeneration due to the normal aging process. As small tears in the disc’s outer layer (annulus) develop and enlarge over time, the jellylike inner layer (nucleus) may bulge outward, causing pressure on the spinal cord and nerves. Occasionally, trauma or an episode of heavy lifting causes sudden rupture of the disc resulting in symptoms.
Summary:
Arm pain and discomfort from a disc herniation can often be resolved with medication and non-operative treatments (physical therapy). When these treatments are successful, arm pain tends to disappear first and it may take longer for weakness or numbness to improve. Surgery is performed for those whose symptoms do not improve.
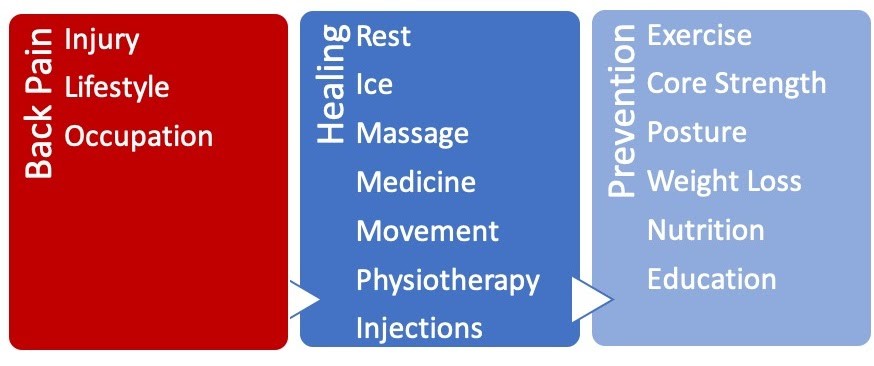
Back Pain
Back pain occurs when the spine is stressed by injury, disease, wear and tear, or poor body mechanics. Acute lower back pain is abrupt, intense pain that settles after a period of days or weeks. It usually resolves with rest and simple self-care measures or occasionally physiotherapy. You have the most important role in the prevention, treatment, and recovery of acute back pain. Rarely, acute lower back pain can persist. Whilst every case is unique, if pain persists for more than a few weeks your GP may arrange investigations to determine the cause or consider referral to a specialist surgeon. Pain that persists for more than 3 months is considered chronic and usually requires further evaluation. Unlike the lower back, thoracic spine pain is less common and usually requires more prompt investigation by your doctor.
Types of Back Pain:
Supporting the weight of your body whilst remaining flexible, the lumbar spine can be prone to injury and pain. Back pain ranges from mild to severe, acute to chronic.
Acute low back pain occurs suddenly and normally heals within several days to a few weeks. Pain is usually started in the muscles, ligaments, joints, or discs. Tight muscles, degenerative discs, and inflamed facet joints are usually the cause but occasionally a trapped nerve may also contribute to the pain.
Chronic back pain is diagnosed when pain lasts for more than 3 months. This may be felt all the time or only with certain activities. Its exact source may be initially hard to determine but may include nerve damage, arthritis, scar tissue or muscle loss. Chronic pain may have an impact on a person’s mental health. Similarly, mental health, stress and anxiety can all have an impact on chronic pain, increasing the intensity of the pain experienced.
Symptoms:
Patients may experience a broad range of symptoms including stiffness, tightness, muscle spasm, aching, stabbing, burning pains. Some experience shooting pains, pressure, or tingling. Pain may radiate and be felt in the buttocks, thighs, or knees. Some may not have any pain felt directly in the back at all. Symptoms are usually more noticeable when bending or arching the back, lifting heavy objects, or if sitting or standing for a long time. You should seek medical help immediately if extreme leg pain or weakness, loss of bladder or bowel function develops, the condition called cauda equina syndrome is a medical emergency.
Causes of Back Pain:
A sedentary lifestyle, excess weight, poor seating, and improper lifting techniques all place stress on the spine and can result in pain. A specific causes of acute lower back pain is only found 20% of the time. Although the specific cause may not be found, some conditions that cause back pain are: • Muscle strain: A sports injury, fall, or strenuous activity can strain muscles. Often when performing out of the ordinary activity. • Osteoarthritis or degenerative disc disease: Both the discs and facet joints involved in spinal motion degenerate with age. Facet joints can become arthritic and the discs may dehydrate, bulge or collapse. • Bulging or herniated disc: The gel-like centre of a spinal disc can bulge or rupture through a weak area in the disc wall. This can cause both back pain and also sciatica • Stenosis: Narrowing of the bony tunnel in the spine that the spinal cord and nerves run through can result in nerve compression. • Rare causes: Very rarely more severe problems can cause back pain. These typically result in a progressive pain that does not self-resolve. These may include fractures, tumours and infections.
Diagnostic Process:
Your complete medical history will be reviewed by your treating doctor including the onset of your pain, aggravating factors and treatments already initiated. The impact on your function and wellbeing will also be considered.
A thorough medical examination will be conducted to help identify the cause and location of your pain along with testing the function of the nervous system that may be involved. Your doctor will also consider causes of pain that may not originate in the spine such as your shoulders, hips, chest or abdomen.
Medical imaging and investigations may be required. Neurospine Institute has developed a close working relationship with leading medical providers. You may be referred for x-rays, a CT scan, MRI, SPECT-CT or nerve conduction testing. Occasionally diagnostic injections may be required.
Treatment Options:
Most back pain can be treated without surgical interventions. The aim is to improve your pain, correct the problem, restore function, and prevent a recurrence.
Self-care: Back pain often resolves with rest, ice, massage, simple pain medication, and gentle stretches. Reducing muscle inflammation and pain using an ice pack during the first 48 hours. A warm shower or heating pack may be used after to relax the muscles. A short period of bed rest is okay, but more than a couple of days can do more harm than good. If your pain is ongoing or recurrent you’ll need to see your doctor.
Medications: Many people get pain relief with over-the-counter anti-inflammatory medications such as ibuprofen or naproxen. Commonly paracetamol may also be used. You should consult with your doctor or pharmacist as to which medication to take. Even common non-prescription medications can have serious side-effects if taken for more than a few days.
Injections: A steroid like Cortisone may be injected directly into the pain source, with the large number of possible pain sources in the spine though identifying which one to inject may be complex.
Physiotherapy: For most back pain, we recommend a nearly normal schedule where pain allows from the onset. Physiotherapy can help you return to full activity as soon as possible and prevent re-injury. You may be referred to a Neurospine Institute Physiotherapist who will assist in both education and training for proper lifting and walking techniques, and exercises to strengthen and stretch your back, legs, and abdominal muscles.
Alternative therapies: Some people may find benefit from alternative therapies such as yoga, pilates, and acupuncture. These treatments may require self-funding and need to be considered on an individual basis. These are not treatments currently offered at Neurospine Institute but their role in your treatment will be considered.
Surgery: Surgery is rarely needed to treat back pain alone, non-surgical measures are usually highly effective. In cases where back pain is present in conjunction with nerve compression or spinal instability, surgery may be required. Every patient is unique, however, in general a focus towards minimally invasive procedures with accelerated rehabilitation protocols is favoured. Surgical decompression or microdiscectomy, artificial disc replacement or fusion may be considered.
Recovery and prevention: Most people with acute low back pain respond to treatment. 80% are symptom-free within 1 to 2 weeks and 90% have recovered within 12 weeks. Maintaining regular activity, a positive mindset and a prompt return to work are all vital. If regular work duties cannot be performed, a period of light duties or reduced hours may be recommended if available in your employment. Typically the longer a patient has off work the longer it will take for them to return to full function. Preventing future back pain is as important as treating the current symptoms. This involves developing safe lifting techniques, correct sitting posture, regular exercise, healthy weight, stress management and mental health along with not smoking.
This group of spinal conditions is very mixed. It includes patients who suffer from any significantly abnormally shaped spine. The group includes patients with Scoliosis and/or Kyphosis and the higher grades of Spondylolisthesis which are usually in children (Spondylolysis and Spondylolisthesis in Children).
It occurs in patients from newborns through infants (Congenital Scoliosis) and adolescents (Scoliosis in Adolescents, Kyphosis in Adolescents) into adulthood and old age. This group of patients are highly complex and require technically demanding operations and Deformity can be a cause of Back Pain in Children. Spine deformity can be caused by Congenital Abnormalities and Syndromes, Trauma, Inflammatory Diseases, Cancers and Metabolic Diseases and their consequences such as Osteoporotic Fracture. Scoliosis in adults and children represent a large category of work for spinal deformity surgeons; more information can be found here.
Tumour
Many different types of ‘Cancer’ can affect the Spine. This includes Benign (non ‘spreading’) tumours, more common in children and young adults, Primary malignant (‘spreading’) tumours of the bones and tissues of the spine themselves (which are quite rare), and the largest group which are the Secondary tumours which are cancers which have spread to the bones of the spine that began somewhere else in the body e.g. breast cancer, prostate cancer, bowel cancer, lung cancer etc.
Secondary, or Metastatic tumours in the spine may cause pain, pressure on nerves, structural instability of the spine or be symptom free.
Their management is complex and often requires a broad range of techniques and medical specialists to be involved. Surgery when necessary is almost always aimed at providing stability to the Spine (Fixation) and at taking pressure off affected nerves (Decompression) as curing the patient of the cancer is unfortunately very rarely possible. This group of patients, particularly those with Multiple Myeloma, Lymphomas and Leukaemia, are often suitable for Percutaneous Spinal Procedures which may allow earlier mobilisation and discharge from hospital and resumption of other cancer treatments.
Infection
Infection of the spine remains quite common.
It is usually a bacterial infection of the intervertebral disc or body of the vertebra which can often be associated with systemic symptoms of fever and high temperature etc along with sometimes very severe back pain. The mainstay of treatment for these patients remains antibiotics but occasionally surgery is necessary. The incidence of tuberculosis in the spine is also increasing in some categories of society.
Inflammatory Diseases
Diseases such as Rheumatoid Arthritis and Ankylosing Spondylitis remain a significant contributor to the spine surgeons’ work load.
The medical management of the diseases has improved remarkably over the last few years and hopefully patients suffering from these conditions needing spine surgery will become far less common for the next generation of spine surgeons. Structural instability in the spine, deformity and nerve compression are common findings in this group of patients.
Lumbar Stenosis
What Is Spinal Stenosis?
Spinal stenosis is a condition caused by the gradual narrowing of the spinal canal through which the nerves of the spinal cord travel.
This narrowing of the spinal canal can happen as a result of the degeneration of both the facet joints and the intervertebral discs. Bone spurs, called osteophytes, grow into the spinal canal. The facet joints can become arthritic and enlarge. The supportive ligaments of the spinal column, especially the ligamentum flavum, thicken with age further narrowing the spinal canal.
These processes narrow the spinal canal, they begin to impinge and put pressure on the nerves roots and spinal cord, creating the symptoms of spinal stenosis.
Stenosis (or Narrowing) may occur in 3 main places:
Central stenosis, where the spinal cord or cauda equina are located,
Lateral recess stenosis, in the tract where the nerve root travel before leaving the spinal canal
Foraminal stenosis, where the individual nerve roots leave the spinal column to travel to the rest of your body.
Some distortion of the spinal canal will occur in virtually every person as they age, but the severity of the symptoms will depend on the size of a person’s spinal canal and the pressure on the nerves. The rate of deterioration varies greatly from person to person, and not everyone will feel symptoms.
Whilst the degenerative or aging process is the most common causes, there are some less common causes of stenosis. These include spondylolisthesis, calcium pyrophosphate crystal deposition, amyloid deposition, and spinal tumors.
What Are The Symptoms Of Spinal Stenosis?
Some people with degenerative disease of the lumbosacral spine may be totally asymptomatic, some may complain of mild discomfort in the low back, and others may not even be able to walk.
Patients who have significant spinal stenosis typically will begin to notice pain in the buttocks, thigh or leg that develops with standing or walking, and improves with rest. In some cases, a patient will complain of leg pain and weakness without having any back pain. More severe symptoms of the disorder include numbness, a tingling sensation and/or weakness in the legs.
Certain positions can alleviate the symptoms of spinal stenosis by relieving pressure on your nerves such as leaning over a walker or shopping cart. Some patients with spinal stenosis can ride a bike and walk up an incline or flight of stairs without any pain. However, if they are walking down an incline or flight of stairs their symptoms may be much worse.
The presentation and severity of the symptoms of spinal stenosis depends on the several factors, including the original width of the spinal canal, the susceptibility of the nerves involved, and the unique functional demands of the patient and the pain tolerance of each individual. If you experience extreme leg weakness (foot drop) or difficulty controlling your bladder or bowel function, seek medical help immediately
Who is affected?
Stenosis affects both men and women and is most common between the ages of 50 and 70. It also may occur in younger people who are born with a narrow spinal canal or who experience an injury to the spine.
How is Spinal Stenosis Diagnosed?
When you first experience pain, consult your family doctor. Your doctor will take a complete medical history to understand your symptoms, any prior injuries or conditions, and determine whether any lifestyle habits are causing the pain. Next a physical exam is performed to determine the source of the pain and test for any muscle weakness or numbness.
Your doctor may order one or more of the following imaging studies: X-ray, MRI scan, myelogram, CT scan, or arterial Doppler study. Based on the results, you may be referred to a neurologist, orthopedist, or neurosurgeon for treatment.
Magnetic resonance imaging (MRI) is a noninvasive test that uses a magnetic field to give a detailed view of the soft tissues of your spine. Nerves and discs are clearly visible. Along with nerve compression, an MRI can also detect bony overgrowth, spinal cord tumors, or infections.
Myelogram is a specialized X-ray where dye is injected into the spinal canal through. An X-ray or CT scan then records the images formed by the dye. Myelograms can show a nerve being pinched by a herniated disc, bony overgrowth, spinal cord tumors, and spinal abscesses. This test may be useful especially if you are unable to have an MRI.
What treatments are available?
Unfortunately there are no medications or physical treatments that can stop or cure spinal stenosis. Non-surgical treatment is the first step to controlling mild to moderate symptoms. If you have severe pain and significant difficulty walking, you may be offered a surgical treatment.
Non-Surgical Treatments:
Self-care:
Using correct posture and keeping your spine in alignment are the most important things you can do for your back. The lower back (lumbar curve) bears most of your weight, so proper alignment of this section can prevent injury to your vertebrae, discs, and other portions of your spine. You may need to make adjustments to your daily standing, sitting, and sleeping habits. You may also need to learn proper ways to lift and bend. You may be able to slow down the progression of stenosis by not smoking and maintaining a weight that’s appropriate for your height and body frame.
Physical Therapy:
The goal of physical therapy is to help you return to full activity as soon as possible. Physical therapists can instruct you on proper posture, lifting, and walking techniques, and they’ll work with you to strengthen your back, leg, and stomach muscles. They’ll also encourage you to stretch and increase the flexibility of your spine and legs. Exercise and strengthening exercises are key elements to your treatment and should become part of your life-long fitness. Check with your doctor before you begin any new exercise program.
Medication:
Nonsteroidal anti-inflammatory drugs (NSAIDs), such as naproxen, ibuprofen, celecoxib or meloxicam may be recommended by your doctor to reduce inflammation and relieve pain. Along with this other pain relief medications may be indicated. Getting the right balance between relieving your symptoms and minimising medication side-effects can be difficult for some patients and may take close work with your doctor.
Steroid injections:
This minimally invasive procedure is performed with x-ray guidance and involves an injection of corticosteroids like cortisone and a numbing agent into the spine. The medicine is delivered directly to the painful area to reduce the swelling and inflammation of the nerves. Repeat injections may be needed to achieve full effect. Duration of pain relief varies, lasting for weeks or years.
Surgical Treatments:
Surgery for spinal stenosis involves decompression of the compressed spinal cord nerves. This may involve removal of the bony and soft tissue overgrowth to relieve pressure and pinching of the spinal nerves. Depending on your symptoms and the area of nerve compression this may also involve spinal fusion surgery.
An example of Lumbar Laminectomy Decompression Surgery
Degenerative Disc Disease
This is the commonest group of clinical problems and is essentially caused by the ‘wear and tear’ changes of ageing and arthritis in the spine. Another name for this is Spondylosis. The usual sorts of symptoms that patients suffer include Low Back Pain or Neck Pain(Arthritis of the Neck), the symptoms of which often come and go in cycles, gradually worsening over time. The other main category of symptom is pain in either the arm or leg which is usually as a result of nerves or even the spinal cord itself being compressed somewhere in the spine. The pain can really be very severe depending upon its cause.
One of the most common is Intervertebral Disc Herniation (or Prolapse) which can occur anywhere in the spine but is most common in the lower lumbar spine and in the lower cervical spine. If the pain is in the legs, this is called Sciatica, if it is in the arms, then it is called Brachalgia. In most cases, the pain will settle down over a few weeks or a month or two and surgical intervention is not needed and Exercises for Low Back Pain treatment can help. In a small proportion the pain is so severe that patients would prefer not to wait a month or two for things to settle down and opt for early surgery, and in some, the pain simply doesn’t settle down after a month or two and then surgery may also be appropriate. In a very small proportion, Disc Prolapse can be an emergency if the disc compromises the nerve function to the bladder, bowel and legs together (Cauda Equina Syndrome).
Other causes of ‘pinched nerves’ in the spine, commonly found in those over fifty years old, are Cervical Myelopathy (when occurring in the neck), and Lumbar Spine Stenosis (when occurring in the back). They have different and complex symptoms but are again typified by symptoms associated with changing or deteriorating nerve function in the arms and/or legs. Lumbar Stenosis is quite frequently accompanied by Degenerative Spondylolisthesis (Spondylolisthesis in Adults) — a medical word that simply means that one vertebra is slipping either forward or backward on another usually due to arthritis changes. Many cases of Degenerative Spondylolisthesis if stable do not need to undergo fusion surgery, but great care must be taken when performing Decompressive Surgery as it can be easy to make the slip worse.Other causes of ‘pinched nerves’ in the spine, commonly found in those over fifty years old, are Cervical Myelopathy (when occurring in the neck), and Lumbar Spine Stenosis (when occurring in the back). They have different and complex symptoms but are again typified by symptoms associated with changing or deteriorating nerve function in the arms and/or legs. Lumbar Stenosis is quite frequently accompanied by Degenerative Spondylolisthesis (Spondylolisthesis in Adults) — a medical word that simply means that one vertebra is slipping either forward or backward on another usually due to arthritis changes. Many cases of Degenerative Spondylolisthesis if stable do not need to undergo fusion surgery, but great care must be taken when performing Decompressive Surgery as it can be easy to make the slip worse.
In general, the results are better for patients with symptoms that are worse in the arms or legs than in the neck or back. Some patients with principally neck or back pain however may be helped by fusion or disc replacement surgery and some patients may be considerably helped by Spinal Injections.
Trauma
Motor vehicle accidents contribute a large proportion and the majority of spinal cord injury happens on the road.
The frequently injured regions of the spine include the Neck and the transitional zone of the spine between the Thoracic and Lumbar spine. Every spine trauma case is different and a wide variety of techniques and approaches may be needed in dealing with them. Posterior and anterior surgery is occasionally necessary. Advances in spinal fixation have revolutionised the management of this group of patients however allowing earlier mobilisation and discharge from hospital for the majority. Less severe injuries such as whiplash can still be troublesome for some time; an excellent information and rehabilitation guide for whiplash sufferers published by the University of Queensland is available here.
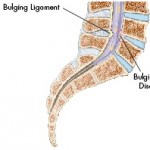
Lumbar Disc Herniation
What Is A Herniated Or Slipped Disc?
Herniation describes an abnormality of the intervertebral disc that is also known as a “slipped,” “ruptured” or “bulging” disc. This occurs when the inner core (nucleus pulposus) of the disc bulges out through the outer layer of ligaments that surround the disc (annulus fibrosis). This tear in the annulus fibrosis causes pain in the back at the point of herniation. If the protruding disc presses on a spinal nerve, the pain may spread to the area of the body that is served by that nerve like the leg.
What Are The Symptoms Of A Herniated Disc?
Usually, the main symptom is sharp, acute pain. In some cases, there may be a previous history of localized low back pain, with pain also extending down the leg served by the affected nerve. This pain is usually described as a deep, sharp or burning, which gets worse as it moves down the affected leg. The onset of pain with a herniated disc may occur suddenly or it may be preceded by a tearing or snapping sensation in the spine, which may be attributed to a sudden rupture in the annulus fibrosis.
How Is A Herniated Disc Diagnosed?
A patient with a herniated disc will usually complain of low back pain that radiates to the leg. They will often have a limitation in range of motion when asked to bend forward or lean backwards, and they may lean to one side as they try to bend forward. Patients will sometimes walk with a painful limp, flexing the affected leg so as not to put too much weight on the side of the body that hurts.
A straight leg raise test may be a positive indication of tension on the nerve root. Abnormalities in the strength and sensation of particular parts of the body may be examined for.
An MRI is the test of choice for diagnosis of a herniated disc, but a CT scan (CAT scan) also may be helpful to indicate where the source of pressure on the nerve root is located.
How Is A Herniated Disc Treated?
Treatment for the vast majority of patients with a herniated disc does not normally include surgery. Most patients will respond to conservative therapy, such as medication, rest and physical therapy.
Surgery is typically recommended only after conservative measures have failed to adequately relieve the symptoms within in a suitable timeframe. Rarely, in the case of severe nerve compression that is possibly causing irreversible damage, surgery may be recommended as a first line of treatment.
The primary element of conservative treatment is controlled physical activity. Usually treatment will begin with a modification of activity and then a gradual return to protected activities. Sitting, bending, lifting and twisting are not beneficial for this condition because they put a large amount of stress and pressure on the lumbar spine, which may increase the pressure on the affected nerve root. The appropriate use of medication is an important part of conservative treatment. This can include anti-inflammatories and specific analgesics your doctor may prescribe. Sometimes an anti-inflammatory or ‘cortisone’ spinal injection for the area of the affected nerve root to lessen swelling and irritation caused by the damaged disc is utilised.
Lumbar/Cervical Discectomy
Anterior cervical discectomy procedures are usually performed to remove pressure on nerves from disc herniations.
A disc herniates when the outer portion of the disc ruptures and some of the softer disc nucleus material squeezes out. The herniated disc pushes against the spinal cord or spinal nerves and tends to cause pain in the neck or arms. Removing the ruptured disc alleviates pressure on the nerves or spinal cord, which usually relieves the pain. A bone graft is usually inserted with instrumentation to keep the disc space at a normal height and fuse the vertebrae above and below the removed disc.
INSICION
An incision is made to one side on the front of the neck. Through this incision, exposure is provided to the front of the cervical spine. The herniated disc that is causing pressure on the spinal nerve is located between vertebrae.
EXCISION
Surgical instruments are used to remove a portion of the herniated disc, which alleviates pressure on the nerve. After disc material is removed, a bone graft is cut to the correct size and placed in between the vertebrae to add stability.
STABILIZATION
A metal plate is placed over the bone graft, and two holes are drilled in each vertebra. Four screws are placed through the plate to secure the plate to the vertebra. The metal plate provides additional support while the bone graft grows in place, fusing the vertebrae.
SUMMARY
The incision is closed and dressed to complete the surgery. Some patients require a cervical collar for a short period of time after surgery. Most patients notice rapid improvement of their arm pain.
Cervical Laminectomy
A cervical laminectomy removes the spinous process and lamina from a vertebra to eliminate pressure on the spinal cord. The source of the pressure is often spinal stenosis, a condition in which there is a narrowing of the spinal canal that causes pressure on the spinal cord or nerves. After removing bone, bone grafts can be added to fuse the vertebrae and provide stability to the spine.
INCISION & REMOVAL
An incision is made along the midline at the back of the neck. After the spine is exposed, surgical instruments are used to remove the spinous process and lamina from the affected vertebrae. Another variation of this step involves using a motorized instrument to cut a trough through the lamina on both sides of the vertebra and removing the lamina and spinous process as a single piece. A surgical microscope is often used during this procedure to ensure a high degree of accuracy.
PREPARING FOR FUSION
A motorized instrument (bur) is used to remove the top (cortical) layer of the articular processes (spine joints) at the sides of the vertebrae to prepare a site for fusing the vertebrae. The fusion will stabilize the spine where bone was removed.
GRAFT PLACEMENT
A motorized instrument (bur) is used to remove the top (cortical) layer of the articular processes (spine joints) at the sides of the vertebrae to prepare a site for fusing the vertebrae. The fusion will stabilize the spine where bone was removed.
SUMMARY
The incision is closed and dressed to complete the procedure. A cervical collar is often worn for 6 weeks following surgery. Patients should be careful to avoid heavy lifting and excessive neck motion during recovery.
Deformity Surgery
Spinal deformity surgery covers a wide range of procedures including surgery for children’s disorders through to the aged spine. In general, it will involve either surgery through the back (posterior surgery) or to the front of the spine (anterior surgery), or a combination of both techniques to achieve an improvement in the overall shape of the spine and in particular, so that the head is balanced over the pelvis both when looking from the front and when looking from the side. Often when a spine deforms, the spinal canal contents (either spinal cord or spinal nerves) are compressed and need to be decompressed or freed during the surgery.
A spinal deformity operation can be a single level operation where only one disc and two bones are operated upon all the way up to fusion from essentially the neck down to the pelvis.
Multi-level deformity surgeries are major operations requiring a large amount of planning and preparation. Usually you will be seen by our physicians and also our physiotherapists for a preoperative stretching and strengthening program, and then again after surgery to monitor your progress and help you to restore function in the weeks and months following surgical intervention.
Spinal deformity surgery is complex and not offered by all surgeons. It is typically a set of procedures with significant risks and therefore should not be undertaken lightly. Some surgeries will take up to 12 hours or more to perform.
If you are being considered for deformity surgery, we are more than happy to put you in touch with patients who have been through deformity surgery themselves so that you can discuss your fears, share your expectations and hear their experience of the process. Often the recovery from this surgery is lengthy.
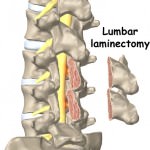
Lumbar Laminectomy for Stenosis
LUMBAR-LAMINECTOMY
A posterior lumbar laminectomy, which is also called a decompression, is done to treat pain caused by degenerative conditions in the lower back. Disc degeneration, bone spurs, and other conditions can cause narrowing and pressure on the spinal nerves (radiculopathy) exiting the spine. A laminectomy procedure removes part of the vertebral lamina to reduce the pressure.
LAMINECTOMY
An incision is made in the middle of the lower back. Surgical instruments are used to remove the spinous processes and lamina. Bone spurs or other sources of spinal nerve compression are also removed. The extra space provided alleviates pressure.
SUMMARY
Patients are often discharged from the hospital after 1-2 days following a lumbar laminectomy. Healing is fairly rapid and back pain from the incision usually subsides within 1-2 weeks.
LUMBAR – LAMINECTOMY, FUSION – INSTRUMENTED
A posterior lumbar laminectomy is done to correct spinal stenosis, which is a narrowing of the spinal canal caused by degenerative conditions in the lower back. Pressure on the spinal nerves (radiculopathy) exiting the spine causes pain, and a laminectomy removes part of the vertebral lamina to reduce the pressure. After removing bone, bone grafts can be added to fuse the vertebrae. In instances where there is instability, instrumentation is added to provide greater stability to the spine.
INCISION & LAMINECTOMY
An incision is made in the middle of the low back. After the spine is exposed, surgical instruments are used to remove the spinous process, lamina, and any bone spurs that may be intruding into the spinal canal. The spinal nerves now have more space with less pressure on them.
PREPARING FOR FUSION
To prepare for the fusion that will stabilize the vertebrae, a motorized instrument is used to remove the top (cortical) layer of the transverse processes. This is the site where the bone grafts for the new fusion will be added.
STABILIZING THE SPINE
Before bone grafts are added, instrumentation is introduced to stabilize the spine. A drill is used to make holes in the pedicle area of the vertebrae, and screws are placed in the drilled holes. Next, rods are positioned between the screws and fastened in place. The rod and screw instrumentation provides stability to the spine and prevents the vertebrae from moving while the bone graft fusion takes place.
BONE GRAFT
Bone grafting can be done with pieces of a patient’s own bone (autograft), processed bone from a bone bank (allograft), or a bone graft substitute (demineralized bone, ceramic extender, or bone morphogenetic protein). To harvest a patient’s own bone for grafting, bone from the iliac crest will typically be removed through the same incision that was made to access the spine. The harvested bone is then placed along the prepared site where the top layer of bone was removed. This bone eventually grows in place, fusing the spine and providing additional stability.
SUMMARY
The incisions are closed and dressed to complete the procedure. Adding the instrumentation to the laminectomy with bone graft fusion increases the strength of the spine directly after surgery, and may decrease the need for a post-operative brace. Patients often remain in the hospital for two to four days following the procedure and should avoid heavy lifting, bending, twisting, and turning for six to twelve weeks.
Minimal Access TLIF
A transforaminal lumbar interbody fusion (TLIF) is performed to remove a portion of a disc that is the source of back or leg pain and fuse the spine. Like the PLIF (posterior lumbar interbody fusion) procedure, bone graft is used to fuse the spinal vertebrae after the disc is removed. However, the TLIF procedure places a single bone graft between the vertebrae from the side, rather than two bone grafts from the rear as in the PLIF procedure. In patients with spinal instability, instrumentation is used to help stabilize the spine during the bone graft fusion. Using a technique known as minimally invasive surgery, this procedure can be done with a much smaller incision than traditional open spinal surgeries and decreases damage to the low back muscles.
ACCESSING THE SPINE
A short incision, approximately 2.5 cm. (1 in.), is made to the side of the middle of the lower back. A device that projects live X-ray images onto a screen, called a fluoroscope is typically used to pinpoint the exact position on the spine where the surgery will be performed. Next, a thin wire or needle is inserted through tissues and muscle to the level of the spine. Special dilators are guided down the wire to separate muscle fibers and provide access to the underlying spine without cutting through the muscles. After the initial dilator is docked on the back of the spine, larger dilators are added, gradually increasing the diameter to allow enough room for the surgical procedure.
RETRACTOR AND INSTRUMENT SET UP
A retractor device that can expand the surgical field and hold back the muscle is placed over the dilators. The dilators are removed and a lighting component is attached to illuminate the surgical field. A hex screwdriver is used to open the retractor blades, holding the soft tissue out of the way. The surgical exposure is now complete. An endoscope or microscope is then added to the edge of the retractor to provide close-up imagery on a screen to help guide the procedure.
ACCESSING THE DISC
Through the opening in the retractor, the surgeon is now able to remove the entire facet joint in order to allow access to the disc. Removing bone here allows the surgeon to access the disc. Excision A grasping instrument is used to remove most of the intervertebral disc. Removing the facet joints and disc relieves pressure on the spinal nerves.
GRAFT PLACEMENT
A single bone graft is placed in the disc space from the lateral (side) aspect through the area exposed where the facet joint was removed. The bone graft will provide stability to the spine when it fuses with the vertebrae above and below it. In variations of this procedure, spacers, cages packed with graft material, or ground bone graft material may also be packed into the disc space to aid with the fusion.
INSTRUMENTATION
Next, the vertebrae are prepared for instrumentation. A sharp awl is used to make holes in the pedicles for insertion of pedicle screws. A guide wire is positioned in the holes and screws are placed over the guide wire and screwed into the pedicle. After the screws have been placed, the guide wire is removed. Next, a rod is positioned between the screws and fastened in place. The rod and screw instrumentation provides stability to the spine and prevents the vertebrae from moving while the bone graft fusion takes place.
SUMMARY
The Minimally Invasive Surgery (MIS) approach to the TLIF procedure can be safely performed with little trauma to the surrounding low back muscles. MIS procedures may result in less postoperative pain, shorter hospitalizations, and quicker patient recovery than traditional open surgical methods.
Motion Preservation Surgery
Motion preservation is a relatively new concept in spine surgery. In suitable patients these procedures can performed as an alternative to spinal fusion surgery. Whilst spinal fusion surgery is often effective in treating pain and other conditions it will cause reduced mobility and can lead to adjacent level disease which sometimes makes it necessary to undergo further surgery in the future. The additional biomechanical stresses that fusion causes on the adjacent spinal motion segments can lead to accelerated degeneration of these adjacent segments. The concept of motion preservation in spine surgery is similar to that of hip or knee replacement surgery where the motion in these joints is preserved by implanting a mobile joint replacement device rather than performing a fusion.
Artificial discs are implants to replace the injured or diseased discs. They are available for cervical and lumbar spinal conditions where patients suffer from neck or back pain due to disc injury or degeneration or from nerve pain in arms or legs.
Some patients are not suitable candidates for artificial disc replacement surgery but might be candidates for posterior motion preservation devices or dynamic fixation. These devices avoid the complete stiffening of a fusion by reducing(but not stopping) the mobility of a diseased spinal motion segment. They can be useful to treat facet joint pain, discogenic pain, spinal canal stenosis and several other conditions. Implants include posterior dynamic stabilisation devices that use flexible rods between spinal stabilisation screws and interspinous spacer implants. Posterior spinous stabilisation devices can also be combined with a spinal fusion to fuse less segments and to avoid or delay adjacent level deterioration in the future.
At the Neurospine Institute we have extensive expertise with these types of surgery and we will always consider motion preservation surgery in an attempt to avoid performing a spinal fusion when possible.
SIJ Fusion/Fixation
SACROILIAC JOINT FUSION
The bony ring of the pelvis is made up of the sacrum and 3 bones that make up the pelvis, the iliac, ischial and pubic bones. The ring is joined at the front by the pubic symphysis. The ring is joined at the back on either side of the sacrum by the sacroiliac joints.
Although the joint only moves by a few degrees in adults, it plays an important role in nearly all physical activities. Almost the entire transmission of force between the upper and lower half of the body takes place via the sacroiliac joints. As with most other moving joints in the human body, degenerative arthritis can develop.
Literature suggests that up to 15-20% of patients presenting with lower back/buttock pain to a spine surgeon’s clinic have symptoms arising from degenerative disease of the sacroiliac joint either alone or in combination with symptomatic lumbar degenerative disease.
Treatment of this condition has been difficult and relatively haphazard partly due to difficulties in accurately diagnosing the condition as well as fairly limited open surgical options for fixation and fusion of the joint.
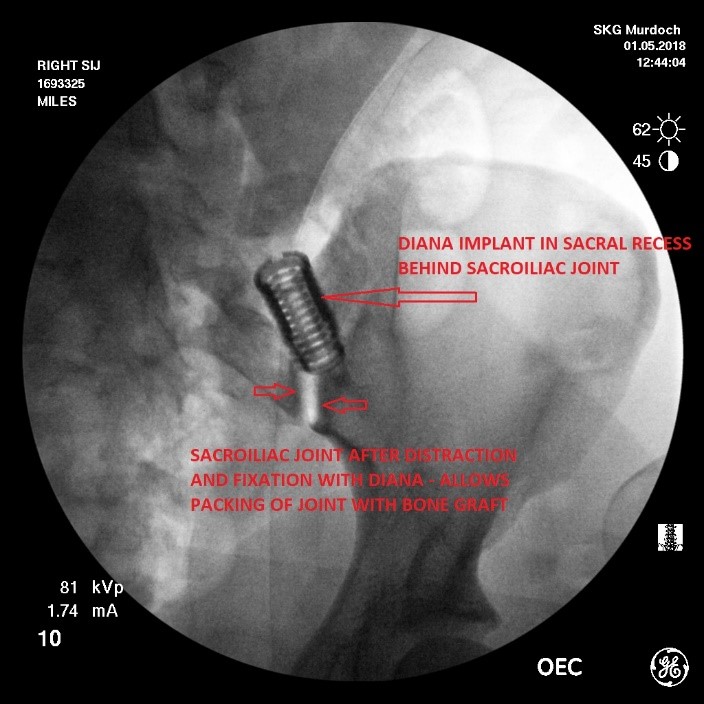
Over the last 5 years there has been an explosion in minimally invasive and mini-open surgical techniques to treat symptomatic degenerative sacroiliac joint disease. One of these procedures is termed the DIANA procedure (Distraction Interference Arthrodesis with Neurovascular Avoidance).
Surgical Technique:
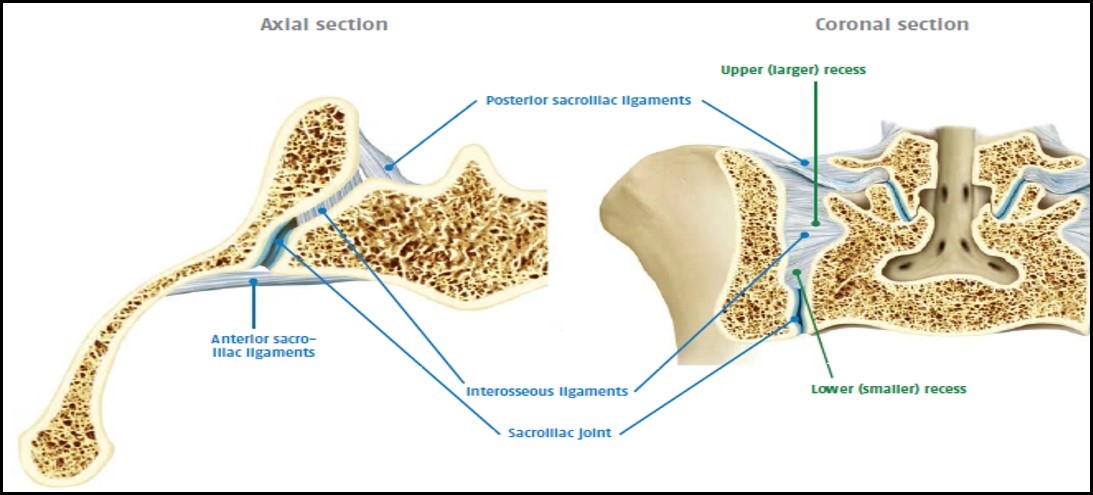
Although the primary goal of the DIANA procedure is stabilisation of the sacroiliac joint, 90% of the procedure itself is actually performed in a large space behind the sacroiliac joint called the sacral recess.
The sacral recess contains multiple strong ligaments (interosseous ligaments) that bridge the gap from the iliac and sacral bones. These ligaments maintain the integrity of the sacroiliac joint and the integrity of connection between the iliac bone of the pelvis and the sacrum.
The DIANA procedure incorporates 4 separate components:
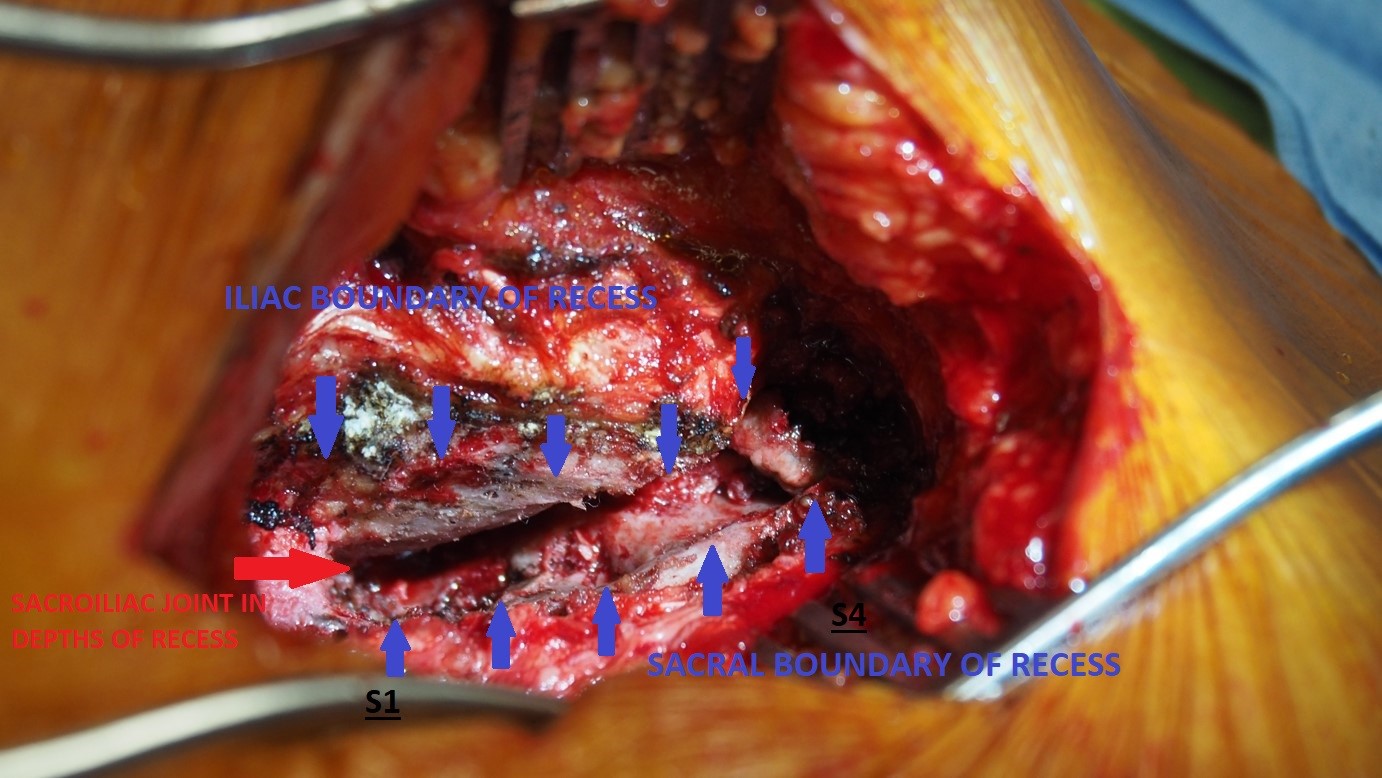
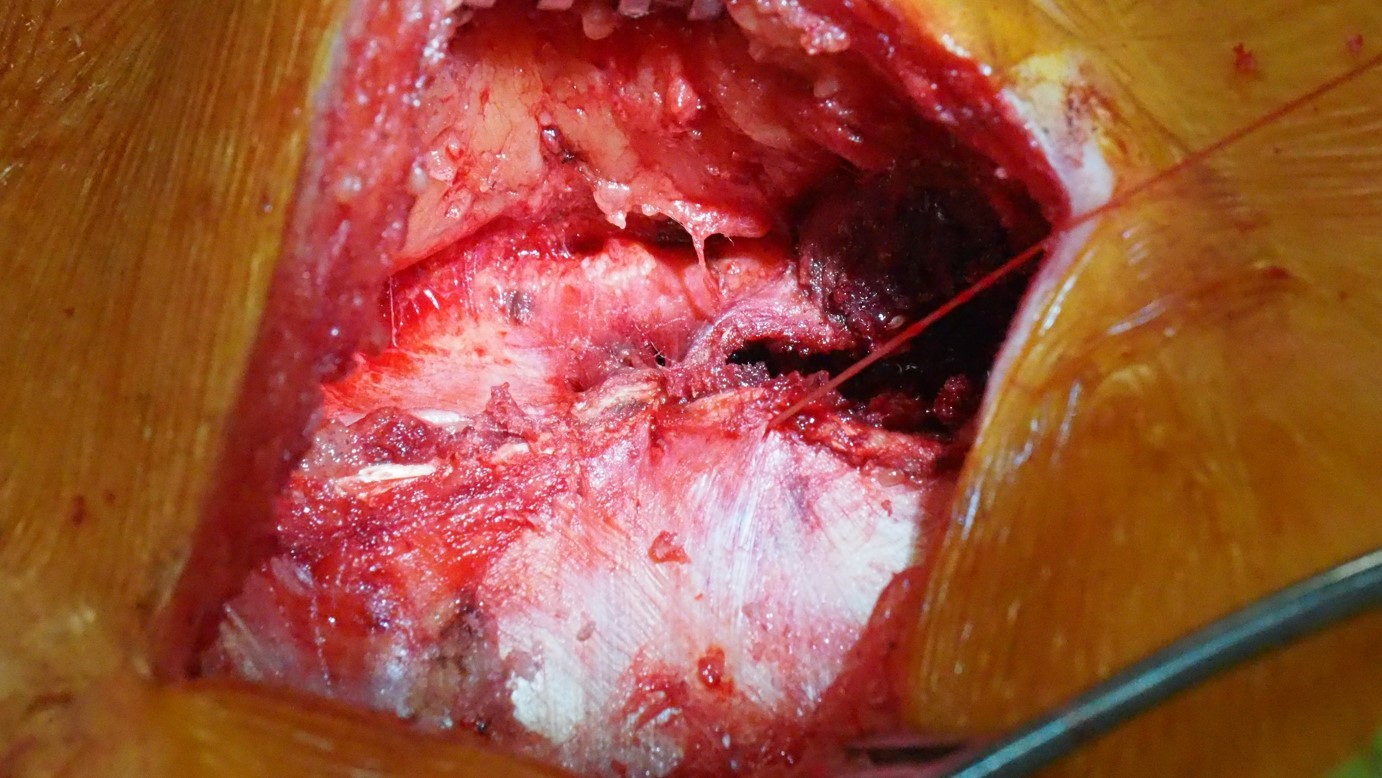
1. Complete exposure of the sacral recess – via a paramedian muscle-splitting incision. The recess is then emptied of soft tissue along this entire extent.
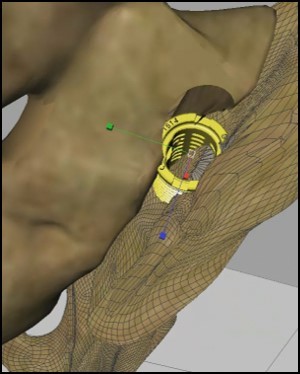
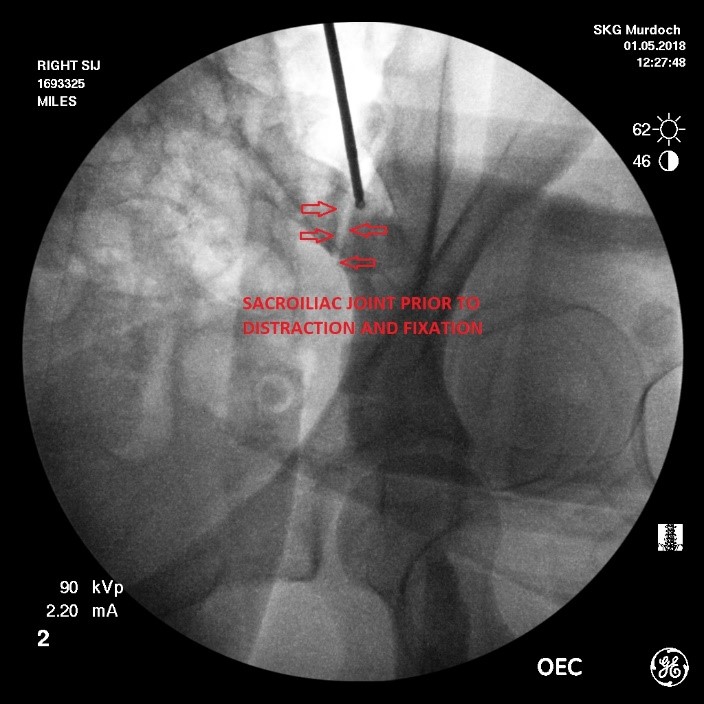
2 & 3. Distraction and fixation of the sacroiliac joint –the sacroiliac joint is indirectly distracted by distracting the medial (sacral) and lateral (iliac) boundaries of the sacral recess. To achieve this a guide pin is implanted using fluoroscopic control into the iliac bone of the pelvis. Positioning and trajectory of the guide pin is an essential component of the procedure and requires careful interpretation of fluoroscopic images performed in the antero-posterior (forward-backward), lateral and oblique planes.
Once the guide pin is positioned correctly and confirmed on the 3 fluoroscopic views, the sacral recess is progressively distracted using a series of progressively larger helical instruments until an appropriate degree of distraction of both the sacral recess and indirectly the underlying sacroiliac joint is achieved.
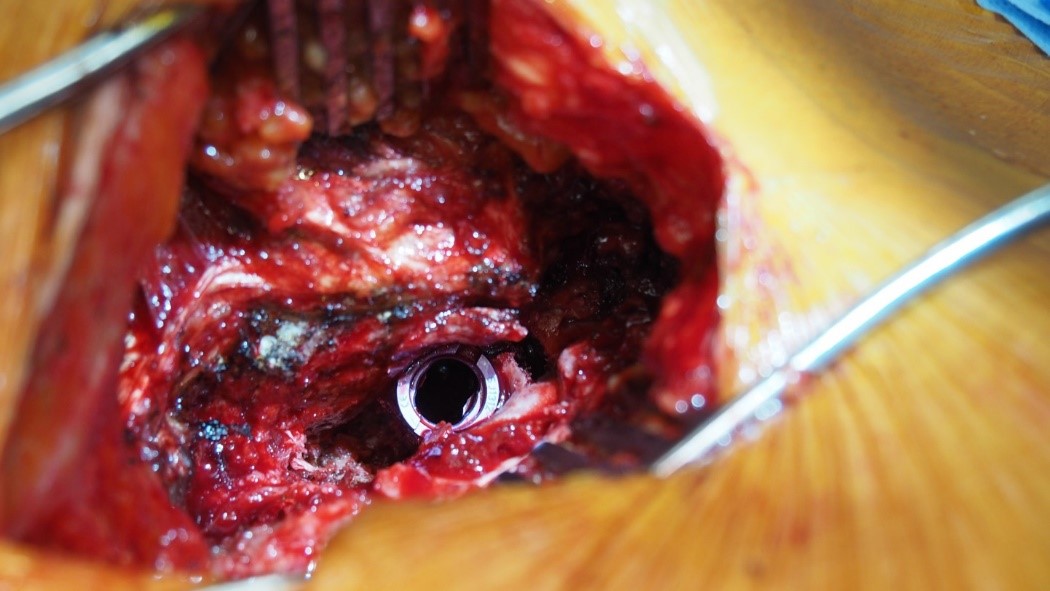
Once a satisfactory degree of distraction of the sacroiliac joint has been achieved,fixation of the distraction must then be obtained. This is achieved by implanting a DIANA screw sized to match the distraction obtained with the helical instruments.
4. Sacroiliac joint fusion – once the sacroiliac joint has been distracted and fixation of the distraction has been obtained by positioning of the DIANA screw, the exposed sacral recess and sacroiliac joint is then packed with bone graft. This component of the procedure is the most essential element of the whole surgery. The progressive development of a solid consolidated fusion mass within the sacral recess over the 6-9 month period after the surgical procedure maintains the distraction/fixation of the sacroiliac joint achieved with implantation of the DIANA screw and painful of the degenerative sacroiliac joint.
Computer Assisted/Neuronavigated Spine Surgery
Surgeons at the Neurospine Institute utilise the most modern Computer Assisted Neuronavigation Devices and intraoperative CT scanners. In spinal surgery this allows for precise implant placement via minimally invasive keyhole approaches minimising muscle and soft tissue trauma. Patients recover quicker and start mobilisation and physiotherapy earlier. The surgeon can obtain a real time update and can verify correct implant position before the patient leaves the operating room making surgery more precise and safe.
The monitor gives guidance to Spine Surgeons Dr Taylor & Cunningham by using the Intra Operative Navigation System